Breast Reconstruction IN BOSTON
BREAST RECONSTRUCTION FOLLOWING BREAST REMOVAL IN BOSTON
Reconstruction of a breast that has been removed due to cancer or other disease is one of the most rewarding surgical procedures available today. New medical techniques and devices have made it possible for surgeons to create a breast that can come close in form and appearance to matching a natural breast. Frequently, reconstruction is possible immediately following breast removal (mastectomy), so the patient wakes up with a breast mound already in place, having been spared the experience of seeing herself with no breast at all.
But bear in mind, post-mastectomy breast reconstruction is not a simple procedure. There are often many options to consider as you and your plastic surgeon should explore what’s best for you.
Currently, Dr. Hein works with breast surgeons at Newton Wellesley Hospital and MetroWest Medical Center to provide immediate reconstruction at the time of mastectomy when indicated.
This information provided on this website will give you a basic understanding of the breast reconstruction procedure – when it’s appropriate, how it’s done, and what results you can expect. It can’t answer all of your questions, since a lot depends on your individual circumstances. During your consultation with Dr. Katherine Hein, ask your questions and concerns if there is anything you don’t understand about the procedure.
WHO IS A CANDIDATE FOR BREAST RECONSTRUCTION?
Most mastectomy patients are medically appropriate for reconstruction, many at the same time that the breast is removed. The best candidates, however, are women whose cancer, as far as can be determined, seems to have been successfully removed by mastectomy.
Still, there are legitimate reasons to wait. Many women aren’t comfortable weighing all the options while they’re struggling to cope with a diagnosis of cancer. Others simply don’t want to have any more surgery than is absolutely necessary. Some patients may be advised by their surgeons to wait, particularly if the breast is being rebuilt in a more complicated procedure using flaps of skin and underlying tissue. Women with other health conditions such as obesity, high blood pressure, or smoking may also be advised to wait.
In any case, being informed of your reconstruction options before surgery can help you prepare for a mastectomy with a more positive outlook for the future.
WHAT ARE STEPS TO PLAN FOR BREAST RECONSTRUCTION SURGERY?
You can begin talking about reconstruction as soon as you’re diagnosed with cancer. Ideally, you’ll want your breast surgeon to work with Dr. Hein as a team to develop a strategy that will put you in the best possible condition for reconstruction.
After evaluating your health, Dr. Katherine Hein will explain which reconstructive options are most appropriate for your age, health, anatomy, tissues, and goals. Be sure to discuss your expectations frankly with Dr. Hein. She will be equally frank with you, describing your options and the risks and limitations of each. Post-mastectomy reconstruction can improve your appearance and renew your self-confidence – but keep in mind that the desired result is improvement, not perfection.
Your surgeon should also explain the anesthesia she will use, the hospital where the surgery will be performed, and the costs. In most cases, health insurance policies will cover most or all of the cost of post-mastectomy reconstruction. Check your policy to make sure you’re covered and to see if there are any limitations on what types of reconstruction are covered.
ALL SURGERY CARRIES SOME UNCERTAINTY AND RISK
Virtually any woman who must lose her breast to cancer can have it rebuilt through reconstructive surgery. But there are risks associated with any surgery and specific complications associated with each procedure.
In general, the usual problems of surgery, such as bleeding, fluid collection, excessive scar tissue, or difficulties with anesthesia can occur, although they’re relatively uncommon. And, as with any surgery, smokers should be advised that nicotine can delay healing, resulting in conspicuous scars and prolonged recovery. Occasionally, these complications are severe enough to require a second operation.
If an implant is used, there is a remote possibility that an infection will develop, usually within the first two weeks following surgery. In some of these cases, the implant may need to be removed for several months until the infection clears. A new implant can later be inserted.
The most common problem, capsular contracture, occurs if the scar or capsule around the implant begins to tighten. This squeezing of the soft implant can cause the breast to feel hard. Capsular contracture can be treated in several ways and sometimes requires either removal or “scoring” of the scar tissue or perhaps removal or replacement of the implant.
Reconstruction has no known effect on the recurrence of disease in the breast, nor does it generally interfere with chemotherapy or radiation treatment, should cancer recur. Your surgeon may recommend continuation of periodic mammograms on both the reconstructed and the remaining normal breast. If your reconstruction involves an implant, be sure to go to a radiology center where technicians are experienced in the special techniques required to get a reliable x-ray of a breast reconstructed with an implant.
Women who postpone reconstruction may go through a period of emotional readjustment. Just as it took time to get used to the loss of a breast, a woman may feel anxious and confused as she begins to think of the reconstructed breast as her own.
WHERE YOUR SURGERY WILL BE PERFORMED
Dr. Hein and her professional staff will give you specific instructions on how to prepare for surgery, including guidelines on eating and drinking, smoking, and taking or avoiding certain vitamins and medications.
While preparing for breast surgery, be sure to arrange for someone to drive you home after your surgery and to help you out for a few days, if needed.
Breast reconstruction usually involves more than one operation. The first stage, whether done at the same time as the mastectomy or later on, is usually performed in a hospital. Follow-up procedures may also be done in the hospital. Or, depending on the extent of surgery required, some procedures can be done in the office.
BREAST RESCONSTRUCTION SURGERY CONSIDERATIONS
Types of Anesthesia
The first stage of reconstruction, creation of the breast mound, is almost always performed using general anesthesia, so you’ll sleep through the entire operation. Follow-up procedures may require only a local anesthesia or local anesthesia combined with a sedative to make you drowsy. You’ll be awake but relaxed and may feel some discomfort.*
Types of Implants
If Dr. Hein recommends the use of an implant, you’ll want to discuss what type of implant should be used. A breast implant is a silicone shell filled with either silicone gel or a salt-water solution known as saline. Commonly, at the time of mastectomy, a temporary implant called a tissue expander is placed. It is gradually filled with fluid in the office, then changed to a traditional implant at a second procedure. (For more information on implants).
WHAT IS THE BREAST RECONSTRUCTION SURGICAL PROCESS?
While there are many options available in post-mastectomy reconstruction, you and your surgeon should discuss the one that’s best for you. Read on to learn more about the two most common breast reconstruction techniques.
Option One: Skin Expansion/Implant
 The most common technique combines skin expansion and subsequent insertion of an implant. A tissue expander is inserted following the mastectomy to prepare for reconstruction. Following mastectomy, Dr. Hein will insert a balloon expander beneath your skin and chest muscle. Through a tiny valve mechanism buried beneath the skin, she will periodically inject a salt-water solution to gradually fill the expander over several weeks or months.*
The most common technique combines skin expansion and subsequent insertion of an implant. A tissue expander is inserted following the mastectomy to prepare for reconstruction. Following mastectomy, Dr. Hein will insert a balloon expander beneath your skin and chest muscle. Through a tiny valve mechanism buried beneath the skin, she will periodically inject a salt-water solution to gradually fill the expander over several weeks or months.*
 After the skin over the breast area has stretched enough, the expander will be removed in a second operation, and a more traditional implant will be inserted. Some patients do not require preliminary tissue expansion before receiving an implant. For these women, Dr. Hein will proceed with inserting a traditional saline or silicone implant at the time of mastectomy.
After the skin over the breast area has stretched enough, the expander will be removed in a second operation, and a more traditional implant will be inserted. Some patients do not require preliminary tissue expansion before receiving an implant. For these women, Dr. Hein will proceed with inserting a traditional saline or silicone implant at the time of mastectomy.
 After surgery, the breast mound is restored. Scars are lasting but will fade with time. The nipple and areola are reconstructed at a later date. More recently, many mastectomies are done while preserving the nipple (“Nipple sparing mastectomy”).* In many of these patients, an implant can be placed at the time of mastectomy, removing the need for tissue expansion and a second surgery. This is known as a “direct to implant” reconstruction.
After surgery, the breast mound is restored. Scars are lasting but will fade with time. The nipple and areola are reconstructed at a later date. More recently, many mastectomies are done while preserving the nipple (“Nipple sparing mastectomy”).* In many of these patients, an implant can be placed at the time of mastectomy, removing the need for tissue expansion and a second surgery. This is known as a “direct to implant” reconstruction.
Option 2: Flap Reconstruction
An alternative approach to implant reconstruction involves creation of a skin flap using tissue taken from other parts of the body, such as the back, abdomen, or buttocks.
 In one type of flap surgery, the tissue remains attached to its original site, retaining its blood supply. The flap, consisting of abdominal skin, fat, and muscle with its blood supply, are tunneled beneath the skin to the chest, creating a pocket for an implant or, in some cases, creating the breast mound itself without need for an implant. This is called a TRAM flap (transverse abdominis musculocutaneous flap).
In one type of flap surgery, the tissue remains attached to its original site, retaining its blood supply. The flap, consisting of abdominal skin, fat, and muscle with its blood supply, are tunneled beneath the skin to the chest, creating a pocket for an implant or, in some cases, creating the breast mound itself without need for an implant. This is called a TRAM flap (transverse abdominis musculocutaneous flap).
With a different flap surgery technique, skin and muscle taken from the back and tunneled to the front of the chest wall to support the reconstructed breast. This is called a latissimus dorsi flap. Most women will also require an implant with this procedure.
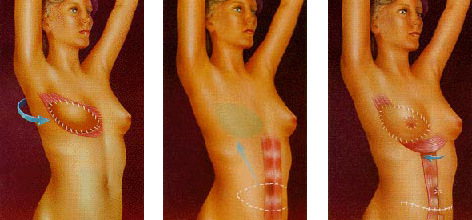 Another flap technique uses tissue that is surgically removed from the abdomen, thighs, or buttocks, and then transplanted to the chest by reconnecting the blood vessels to new ones in that region. This procedure requires the skills of a plastic surgeon who is experienced in microvascular surgery as well. This type of surgery is generally only performed at tertiary care centers.
Another flap technique uses tissue that is surgically removed from the abdomen, thighs, or buttocks, and then transplanted to the chest by reconnecting the blood vessels to new ones in that region. This procedure requires the skills of a plastic surgeon who is experienced in microvascular surgery as well. This type of surgery is generally only performed at tertiary care centers.
Regardless of whether the tissue is tunneled beneath the skin on a pedicle or transplanted to the chest as a microvascular flap, this type of surgery is more complex than skin expansion. Scars will be left at both the tissue donor site and at the reconstructed breast, and recovery will take longer than with an implant.* On the other hand, when the breast is reconstructed entirely with your own tissue, the results are generally more natural and there are no concerns about a breast implant. In some cases, you may have the added benefit of an improved abdominal contour.
FOLLOW-UP PROCEDURES
Most breast reconstruction involves a series of procedures that occur over time. Usually, the initial reconstructive operation is the most complex. Follow-up surgery may be required to replace a tissue expander with an implant or to reconstruct the nipple and the areola. Many surgeons recommend an additional operation to enlarge, reduce or lift the natural breast to match the reconstructed breast. This procedure may leave scars on an otherwise normal breast and may not be covered by insurance.
WHAT IS THE RECOVERY PROCESS AFTER BREAST RECONSTRUCTION SURGERY?
You are likely to feel tired and sore for a week or two after reconstruction. Most of your discomfort can be controlled by medication prescribed by your doctor.*
Depending on the extent of your surgery, you’ll probably be released from the hospital in two to five days. Many reconstruction options require a surgical drain to remove excess fluids from surgical sites immediately following the operation, but these are removed within the first week or two after surgery. Most stitches are removed in a week to ten days. Scars at the breast, nipple and abdomen will fade substantially with time but may never disappear entirely.*
GETTING BACK TO NORMAL
It may take you up to six weeks to recover from a combined mastectomy and reconstruction or from a flap reconstruction alone. If implants are used without flaps or reconstruction is done apart from the mastectomy, your recovery time will be shorter.*
Reconstruction cannot restore normal sensation to your breast, but in time, some feeling may return. Most scars will fade substantially over time, though it may take as long as one to two years, but they’ll never disappear entirely.* The better the quality of your overall reconstruction, the less distracting you’ll find those scars.
Follow your surgeon’s advice on when to begin stretching exercises and normal activities. As a general rule, you’ll want to refrain from any overhead lifting, strenuous sports and sexual activity for three to six weeks following reconstruction.*
YOUR NEW LOOK
Chances are your reconstructed breast may feel firmer and look rounder or flatter than your natural breast. It may not have the same contour as your breast before mastectomy, nor will it exactly match your opposite breast. But these differences will be apparent only to you. For most mastectomy patients, breast reconstruction dramatically improves their appearance and quality of life following surgery.
Click here for more information about Breast Reconstruction.
WHY YOU SHOULD SELECT ACCURATE AESTHETICS FOR YOUR BREAST RECONSTRUCTION SURGERY
![]() Dr. Katherine Hein is among the top cosmetic surgeons in the Boston, MetroWest, Wellesley, and Sudbury area. Dr. Hein is certified by the American Board of Plastic and Reconstructive Surgery and has specialized in breast and cosmetic surgery since 1999. She has performed thousands of cosmetic and reconstructive surgeries.
Dr. Katherine Hein is among the top cosmetic surgeons in the Boston, MetroWest, Wellesley, and Sudbury area. Dr. Hein is certified by the American Board of Plastic and Reconstructive Surgery and has specialized in breast and cosmetic surgery since 1999. She has performed thousands of cosmetic and reconstructive surgeries.
When you select Accurate Aesthetics Plastic Surgery for your breast reconstruction procedure you can be reassured of a close personal relationship with Dr. Hein and her professional staff.
*Results may vary and are not guaranteed. Consult with the medical professionals at Accurate Aesthetics Plastic Surgery to see if you are a candidate.

Discover how Dr. Hein can help you achieve your
desired goals by scheduling a private consultation